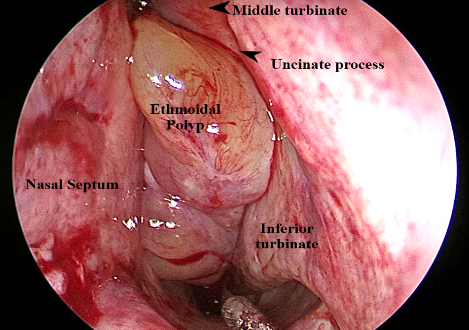
Ethmoidal polyps are multiple, bilateral, painless, pearly white, grape like masses arising from the ethmoidal air cells.
In early stages, nasal polyp is covered by ciliated columnar epithelium like that of normal nasal mucosa but later it converts to transitional and squamous type on exposure to atmospheric irritants.
Submucosa shows large intercellular spaces filled with serous fluid. There is also infiltration with eosinophils and round cells. These polyps are multiple, bilateral and have a grape like appearance. They have a strong allergic co-relation.